
Turning Commitments into Action: Key Takeaways from the 11th World Heart Summit and the 2026 Congenital Heart Disease Report
The global health community gathered at the Biotech Campus in Geneva, Switzerland, on May 16–17, 2026, for the 11th World Heart Summit. The summit's core mission focused on actionable policy changes, healthcare access equity, and transitioning the global heart community from making declarations to implementing concrete solutions.Convened by the World Heart Federation (WHF) just ahead of the 79th World Health Assembly, this year’s summit stood out as a critical pivot point in global health diplomacy. The central theme of the event was clear: the time for high-level political declarations has passed, and the era of concrete, scalable, and well-funded national action plans must begin.
Bringing together health ministers, clinical experts, commercial stakeholders, and civil society leaders, the two-day summit tackled the structural, financial, and environmental forces shaping cardiovascular health worldwide. Most notably, the event marked the launch of the landmark World Heart Report 2026, which cast a much-needed spotlight on a long-neglected crisis: Congenital Heart Disease (CHD).
The Launch of the World Heart Report 2026: Confronting Pediatric Heart Health "Deserts"
Every year, millions of families face the devastating reality of a Congenital Heart Disease diagnosis. As structural abnormalities of the heart or great vessels present at birth, CHD impacts roughly 1.4% to 2.3% of all infants born globally. In 2023 alone, an estimated 2.3 million children were born with the condition.
The launch of the latest findings at the summit underscored a stark, tragic inequity: over 90% of children in low- and middle-income countries (LMICs) live in pediatric heart health "deserts" with virtually no access to timely cardiovascular care.
While a child born with critical or moderate CHD in a high-income nation can benefit from neonatal stabilization, advanced imaging, and life-saving corrective surgeries, the reality in resource-limited settings is grim. Without timely intervention, the most severe forms of CHD are fatal in up to 85% of infants. The report reveals that the age-standardized mortality rate for CHD in low-income regions is four times higher than in high-income countries.
Crucially, the report and surrounding panels emphasized that CHD is no longer just a pediatric issue; it is a lifelong condition. Thanks to medical advances, a growing cohort of patients are surviving into adulthood, requiring highly nuanced, multidisciplinary care throughout their lives. To address this crisis, the WHF issued an urgent call to action for governments to:
Build Workforce Capacity: Invest heavily in training and retaining a dedicated pediatric and congenital cardiac workforce.
Eradicate Social Stigma: Launch public health campaigns to counter cultural misconceptions surrounding birth defects.
Bridge the Data Gap: Improve national surveillance and epidemiological data to accurately track CHD determinants and outcomes.
The complete text, data visualizations, and strategic frameworks are available directly through the World Heart Report 2026: Congenital Heart Disease.
Building Workforce Capacity: Operationalizing the Layered Ecosystem of Care
The summit’s core mandate—to build workforce capacity and preserve the specialized workforce—demands more than just graduating a higher volume of cardiothoracic surgeons. A specialist cannot repair a transposition of the great arteries or a hypoplastic left heart if the fragile patient does not survive the initial triage window in a rural clinic or general ward. To turn this mandate into clinical reality, health systems must integrate standard resuscitation frameworks into a structured, tiered strategy.
Specialized pediatric resuscitation skillsets serve as the precise clinical machinery that operationalizes the World Heart Federation's call to action. By introducing standardized certification pipelines, health ministries can build an overlapping safety net that spans from community clinics to advanced tertiary intensive care units.
Stratifying Competence: PEARS vs. PALS
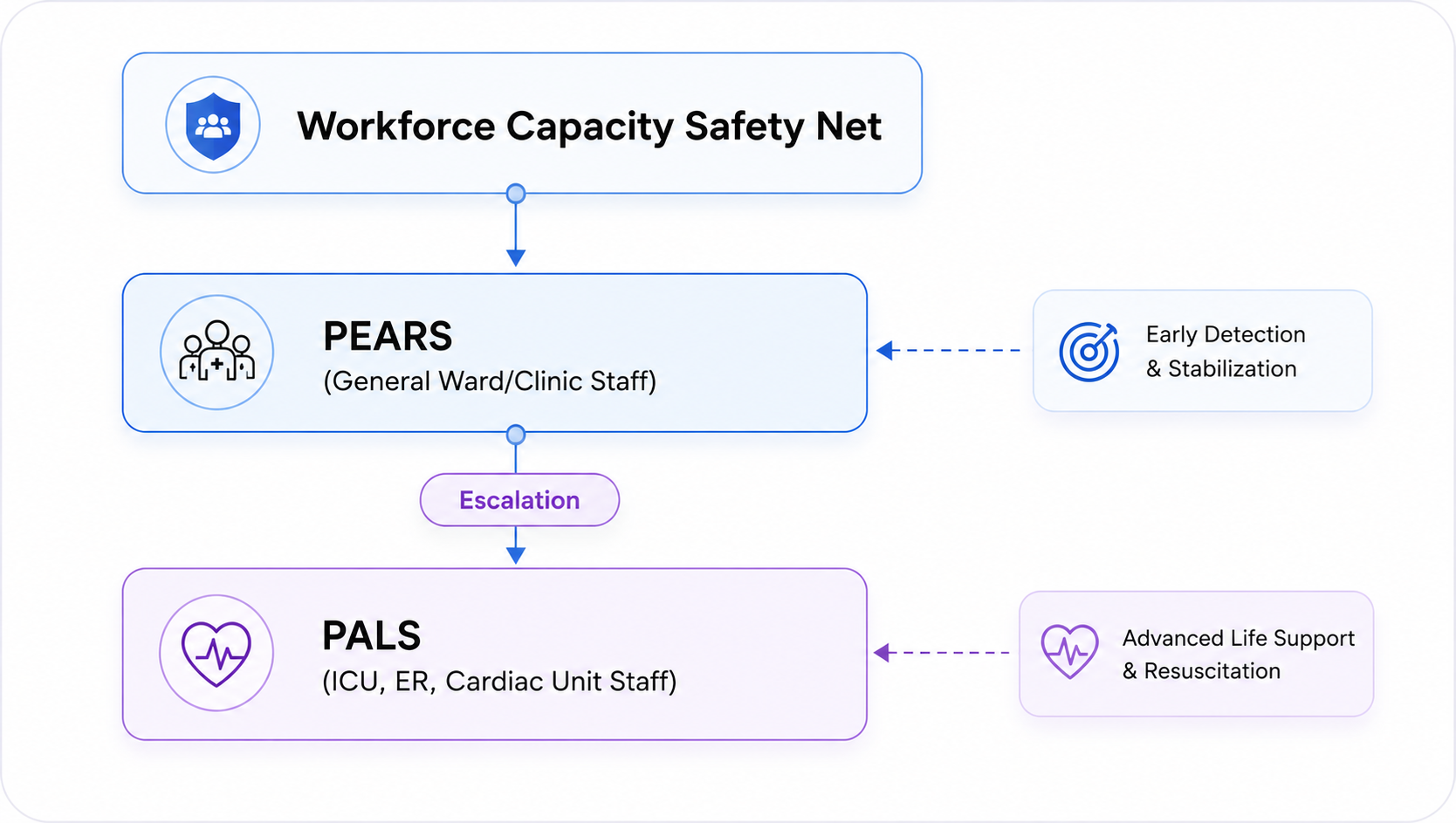
Rather than exhausting finite educational resources attempting to train every general health worker in specialized cardiology, a sustainable system stratifies competence using targeted training frameworks. This architecture establishes two crucial lines of defense:
PEARS (Pediatric Emergency Assessment, Recognition, and Stabilization): Deployed across general ward nurses, community clinics, and outpatient personnel. This framework focuses heavily on early identification of respiratory failure and shock before cardiac arrest occurs.
PALS (Pediatric Advanced Life Support): Mandated for the dedicated cardiac workforce, ER staff, and ICUs. This framework governs advanced interventions, cardiac rhythm management, intraosseous access, and team-led resuscitation.
The integration of PEARS ensures that the broad, non-specialized healthcare workforce acts as an intelligent radar system. Pediatric patients with fragile congenital anatomy frequently experience sudden, severe metabolic decompensation. PEARS empowers a bedside nurse or rural practitioner to recognize the subtle warning signs of impending circulatory collapse—such as altered mental status, poor peripheral perfusion, or respiratory distress—and initiate aggressive stabilization measures long before a code blue is ever declared.
Once a patient is stabilized or escalated, PALS provides the specialized workforce with an advanced, universal operational language. In high-stress resuscitation environments, a shared algorithm minimizes cognitive load, standardizes drug dosages, and structures team communication. This coordinated approach is vital for congenital heart disease patients, whose underlying structural anomalies require rapid, precise clinical decisions.
Navigating Complex Congenital Pathologies
Standard resuscitation guidelines are predicated on standard, four-chambered cardiovascular anatomy. However, congenital anomalies rewrite the physiological rules of life support. Infants navigating single-ventricle palliation (such as a Norwood or Glenn physiology) or complex shunts react atypically to standard algorithms. For example, administering unmonitored high-flow oxygen can alter pulmonary vascular resistance, trigger systemic hypoperfusion, and precipitate acute cardiovascular collapse.
A workforce trained systematically in PALS gains the baseline algorithmic discipline required to comprehend these critical physiological exceptions. Advanced life support training provides the foundation upon which clinicians learn to adjust fluid resuscitation volumes, modulate oxygen delivery, and manage complex arrhythmias unique to the congenital population. Without this foundation, specialized care plans cannot be executed safely.
Fostering Workforce Competence and Retention
The World Heart Summit explicitly paired the imperative to train a workforce with the necessity to retain it. Chronic clinical burnout in pediatric cardiology and intensive care is heavily driven by moral injury—the profound psychological trauma experienced by healthcare workers when they feel ill-equipped during a crisis.
Systematically investing in high-fidelity simulation and ongoing PEARS and PALS certification directly alters this dynamic. Transforming a high-stress medical crisis into a predictable, well-rehearsed workflow shifts institutional culture from a state of panic to one of clinical competence. When frontline clinicians and specialized staff feel structurally supported, psychologically secure, and technically capable of protecting their patients, long-term workforce retention follows naturally.
To review the milestone discussions and closing consensus from Geneva on advancing universal health coverage and turning global policy into community-level action, watch the World Heart Summit 2026 Highlights video.
ACLS Academy is an American Heart Association-aligned Training Center and All-Star award recipient providing emergency response and healthcare training courses throughout Greater Boston, including locations in Quincy, Bridgewater, and Newton Centre. Course offerings include CPR and AED training, BLS, ACLS, PALS, PEARS, ACLS-EP, ASLS, TNCC, ENPC, NRP, First Aid, Bloodborne Pathogens training, and instructor certification courses for healthcare professionals, workplaces, schools, and community organizations. . Browse our catalogue of courses.